

AAV gene transfer delays disease onset in a TPP1-deficient canine model of the late infantile form of Batten disease
- PMID: 26560358
- PMCID: PMC4968409
- DOI: 10.1126/scitranslmed.aac6191
AAV gene transfer delays disease onset in a TPP1-deficient canine model of the late infantile form of Batten disease
Abstract
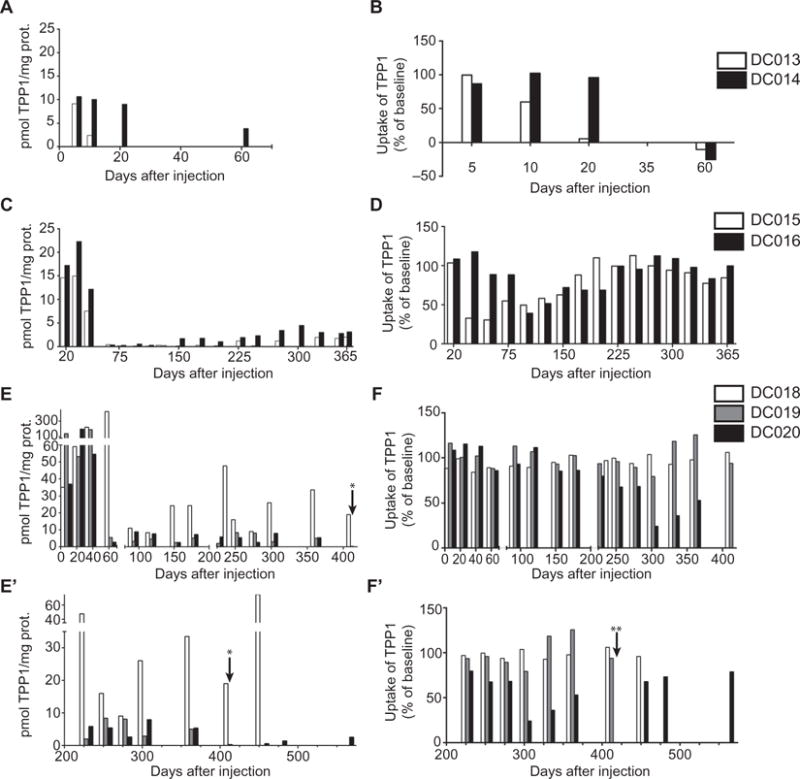
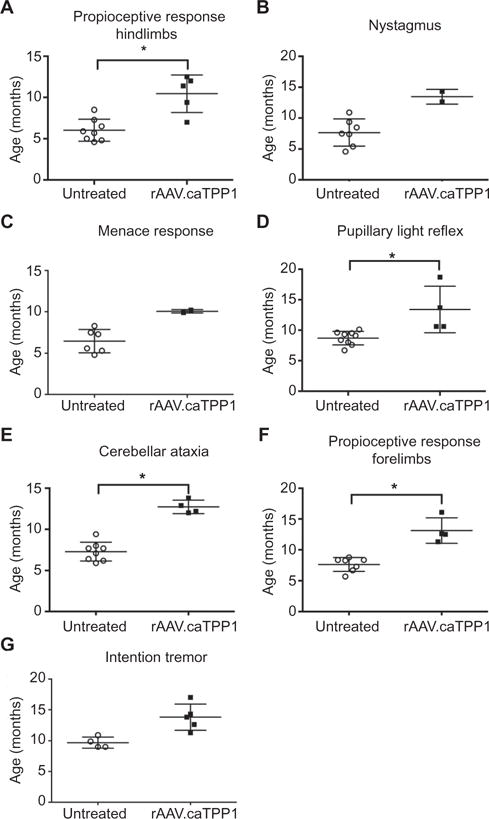
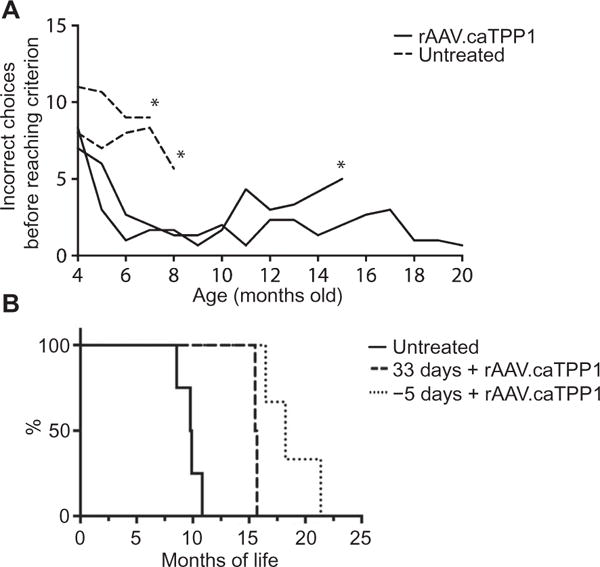
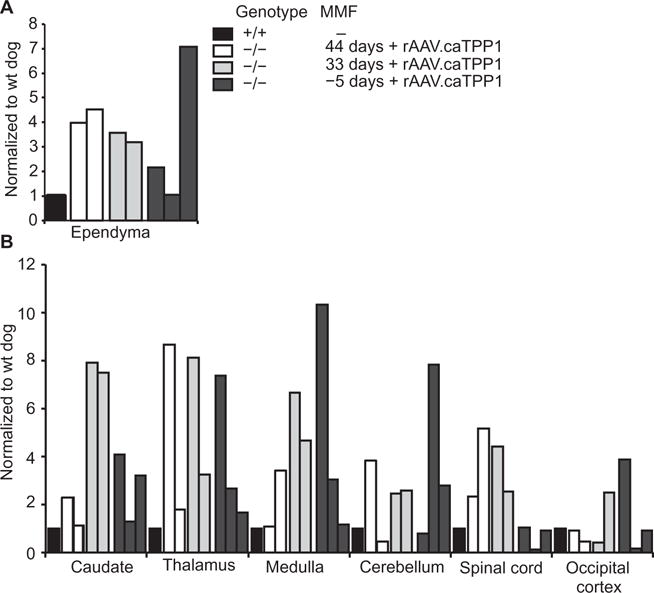
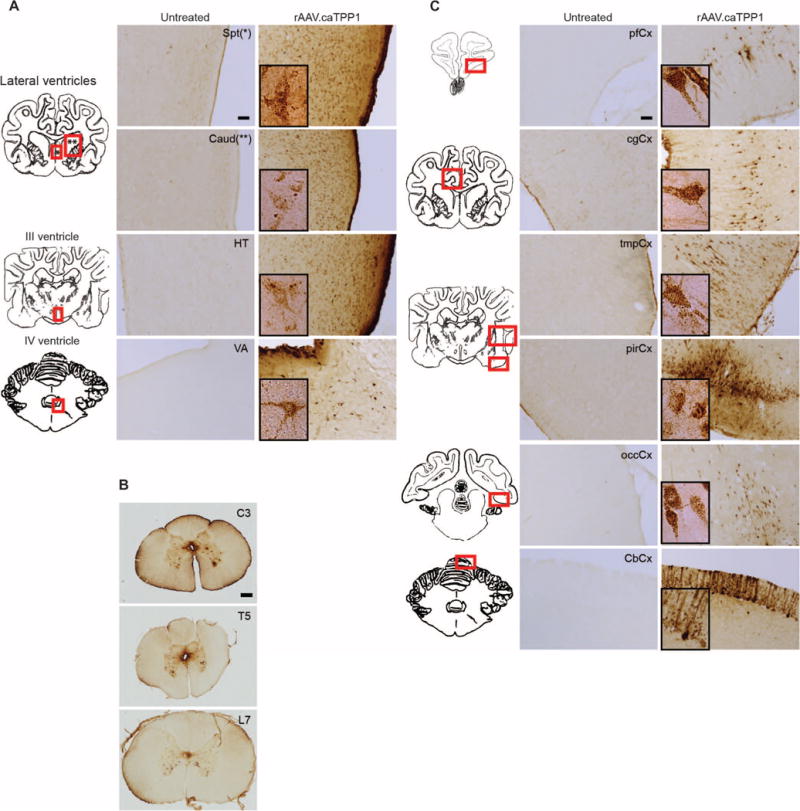
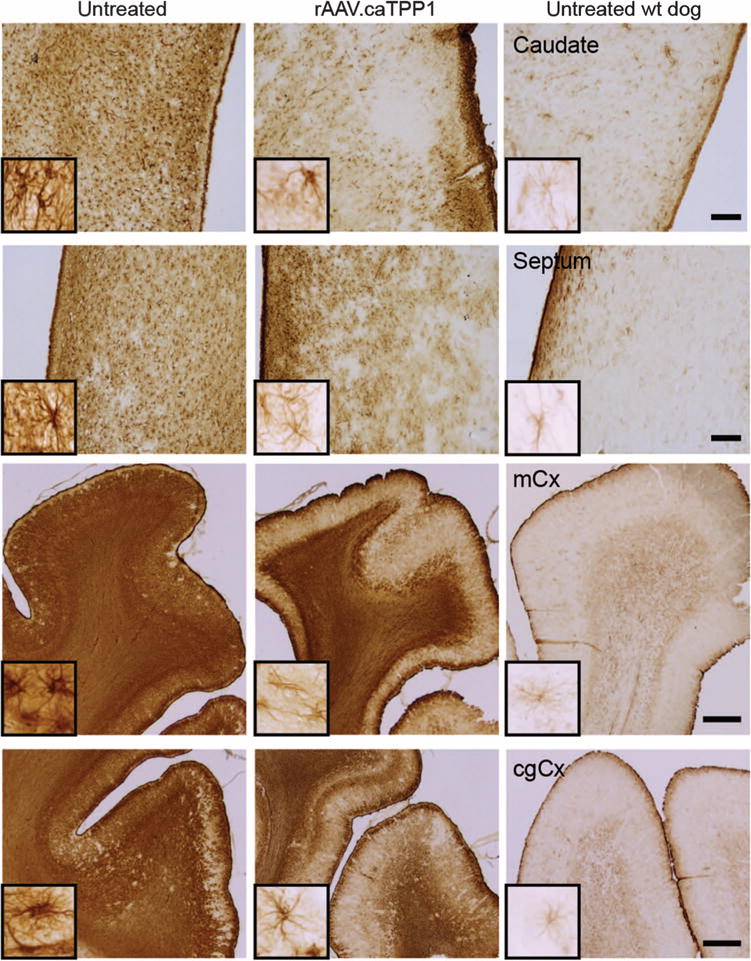
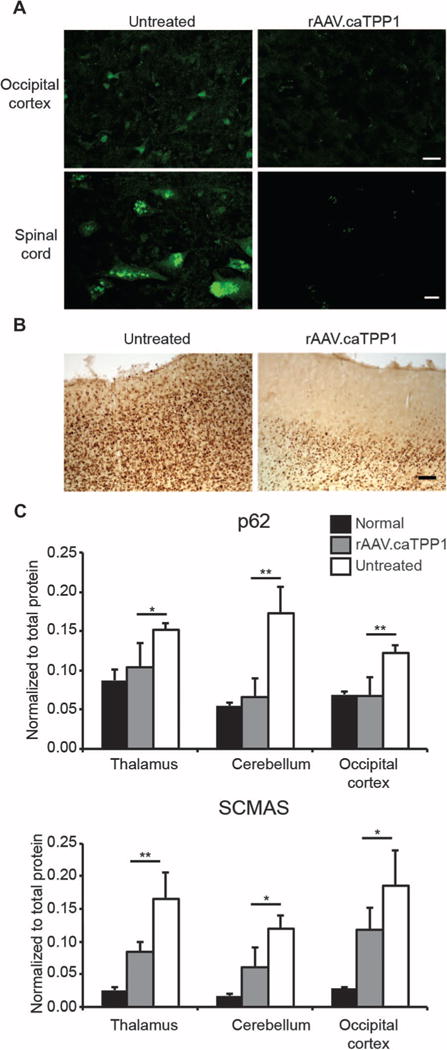
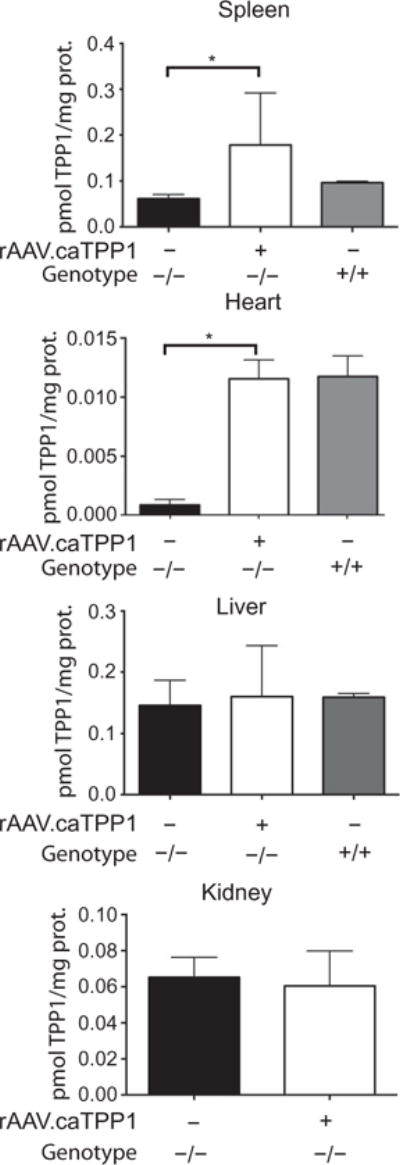
The most common form of the childhood neurodegenerative disease late infantile neuronal ceroid lipofuscinosis (also called Batten disease) is caused by deficiency of the soluble lysosomal enzyme tripeptidyl peptidase 1 (TPP1) resulting from mutations in the TPP1 gene. We tested whether TPP1 gene transfer to the ependyma, the epithelial lining of the brain ventricular system, in TPP1-deficient dogs would be therapeutically beneficial. A one-time administration of recombinant adeno-associated virus (rAAV) expressing canine TPP1 (rAAV.caTPP1) resulted in high expression of TPP1 predominantly in ependymal cells and secretion of the enzyme into the cerebrospinal fluid leading to clinical benefit. Diseased dogs treated with rAAV.caTPP1 showed delays in onset of clinical signs and disease progression, protection from cognitive decline, and extension of life span. By immunostaining and enzyme assay, recombinant protein was evident throughout the brain and spinal cord, with correction of the neuropathology characteristic of the disease. This study in a naturally occurring canine model of TPP1 deficiency highlights the utility of AAV transduction of ventricular lining cells to accomplish stable secretion of recombinant protein for broad distribution in the central nervous system and therapeutic benefit.
Copyright © 2015, American Association for the Advancement of Science.
Conflict of interest statement
Figures
Comment in
-
A canine model for neuronal ceroid lipofuscinosis highlights the promise of gene therapy for lysosomal storage diseases.Ann Transl Med. 2016 Oct;4(Suppl 1):S20. doi: 10.21037/atm.2016.10.16. Ann Transl Med. 2016. PMID: 27867988 Free PMC article. No abstract available.
Similar articles
-
Extraneuronal pathology in a canine model of CLN2 neuronal ceroid lipofuscinosis after intracerebroventricular gene therapy that delays neurological disease progression.Gene Ther. 2017 Apr;24(4):215-223. doi: 10.1038/gt.2017.4. Epub 2017 Feb 2. Gene Ther. 2017. PMID: 28079862 Free PMC article.
-
Enzyme replacement therapy attenuates disease progression in a canine model of late-infantile neuronal ceroid lipofuscinosis (CLN2 disease).J Neurosci Res. 2014 Nov;92(11):1591-8. doi: 10.1002/jnr.23423. Epub 2014 Jun 17. J Neurosci Res. 2014. PMID: 24938720 Free PMC article.
-
CLN2 Disease (Classic Late Infantile Neuronal Ceroid Lipofuscinosis).Pediatr Endocrinol Rev. 2016 Jun;13 Suppl 1:682-8. Pediatr Endocrinol Rev. 2016. PMID: 27491216 Review.
-
Enzyme replacement therapy delays pupillary light reflex deficits in a canine model of late infantile neuronal ceroid lipofuscinosis.Exp Eye Res. 2014 Aug;125:164-72. doi: 10.1016/j.exer.2014.06.008. Epub 2014 Jun 19. Exp Eye Res. 2014. PMID: 24954537
-
Homozygous missense TPP1 mutation associated with mild late infantile neuronal ceroid lipofuscinosis and the genotype-phenotype correlation.Seizure. 2019 Jul;69:180-185. doi: 10.1016/j.seizure.2018.08.027. Epub 2018 Sep 2. Seizure. 2019. PMID: 31059981
Cited by
-
Evaluation of neuroretina following i.v. or intra-CSF AAV9 gene replacement in mice with MPS IIIA, a childhood dementia.CNS Neurosci Ther. 2024 Aug;30(8):e14919. doi: 10.1111/cns.14919. CNS Neurosci Ther. 2024. PMID: 39123298 Free PMC article.
-
Ependymal cells: roles in central nervous system infections and therapeutic application.J Neuroinflammation. 2024 Oct 9;21(1):255. doi: 10.1186/s12974-024-03240-2. J Neuroinflammation. 2024. PMID: 39385253 Free PMC article. Review.
-
Mice deficient in the lysosomal enzyme palmitoyl-protein thioesterase 1 (PPT1) display a complex retinal phenotype.Sci Rep. 2019 Oct 2;9(1):14185. doi: 10.1038/s41598-019-50726-8. Sci Rep. 2019. PMID: 31578378 Free PMC article.
-
Longitudinal In Vivo Monitoring of the CNS Demonstrates the Efficacy of Gene Therapy in a Sheep Model of CLN5 Batten Disease.Mol Ther. 2018 Oct 3;26(10):2366-2378. doi: 10.1016/j.ymthe.2018.07.015. Epub 2018 Jul 17. Mol Ther. 2018. PMID: 30078766 Free PMC article.
-
Early postnatal administration of an AAV9 gene therapy is safe and efficacious in CLN3 disease.Front Genet. 2023 Mar 24;14:1118649. doi: 10.3389/fgene.2023.1118649. eCollection 2023. Front Genet. 2023. PMID: 37035740 Free PMC article.
References
-
- Chang M, Cooper JD, Davidson BL, van Diggelen OP, Elleder M, Goebel HH, Golabek AA, Kida E, Kohlschütter A, Lobel P, Mole SE, Schulz A, Sleat DE, Warburton M, Wisniewski KE. The Neuronal Ceroid Lipofuscinoses (Batten Disease) Oxford Univ Press; New York: Contemporary Neurology Series. 2011. pp. 80–109.
-
- Sleat DE, Donnelly RJ, Lackland H, Liu CG, Sohar I, Pullarkat RK, Lobel P. Association of mutations in a lysosomal protein with classical late-infantile neuronal ceroid lipofuscinosis. Science. 1997;277:1802–1805. - PubMed
-
- Sohar I, Sleat DE, Jadot M, Lobel P. Biochemical characterization of a lysosomal protease deficient in classical late infantile neuronal ceroid lipofuscinosis (LINCL) and development of an enzyme-based assay for diagnosis and exclusion of LINCL in human specimens and animal models. J Neurochem. 1999;73:700–711. - PubMed
-
- Sands MS, Davidson BL. Gene therapy for lysosomal storage diseases. Mol Ther. 2006;13:839–849. - PubMed
-
- Ichimura T, Fraser PA, Cserr HF. Distribution of extracellular tracers in perivascular spaces of the rat brain. Brain Res. 1991;545:103–113. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
