
Abstract
The global incidence of hyperuricemia is increasing in parallel with rising obesity rates. This study investigated the relationship between weight change patterns and the risk of hyperuricemia. Utilizing data from the NHANES, we conducted a retrospective cohort analysis of 20,545 U.S. adults aged 40–75 years. We categorized weight changes into six patterns based on BMI measurements at baseline and 10 years prior. Hyperuricemia was defined as uric acid ≥ 7.0 mg/dL in males and ≥ 6.0 mg/dL in females. Multivariable logistic regression models were used to assess the associations between weight change patterns and hyperuricemia. Participants with weight gain or obesity had significantly higher odds of hyperuricemia (ORs = 2.32 [95% CI: 1.93–2.80, P < 0.001] to 4.72 [95% CI: 3.95–5.63, P < 0.001]). Those transitioning from obese to normal weight had reduced odds of hyperuricemia (OR = 0.41 [95% CI: 0.21–0.79, P = 0.008]). A nonlinear relationship between BMI percentage change and hyperuricemia was observed, with a change of ≥ 6% associated with a higher OR of 6.72 (95% CI 3.76–12.02, P < 0.001). The impact was more pronounced in females. This study provides evidence for a significant nonlinear relationship between weight change and hyperuricemia, emphasizing the need for gender-specific, tailored weight management strategies.
Similar content being viewed by others


Introduction
Hyperuricemia, defined as elevated uric acid levels in the blood, is a key biochemical basis for developing gout1. In recent years, with changes in lifestyle and the prevalence of obesity, the incidence of hyperuricemia has been increasing globally2. Chronic hyperuricemia not only leads to gout but is also associated with various metabolic diseases such as hypertension, cardiovascular diseases, and chronic kidney disease, posing a serious threat to human health3,4.
Obesity significantly contributes to hyperuricemia, a condition characterized by elevated uric acid levels in the blood. Research indicates that increased body mass index (BMI) and waist circumference (WC), along with general and abdominal obesity, are significant risk factors for hyperuricemia. These associations are particularly pronounced in women, younger adults, and individuals without diabetes mellitus5. The study revealed that obesity precedes hyperuricemia, with baseline obesity significantly predicting the risk of incident hyperuricemia. Elevated uric acid partially mediates the relationship between obesity and hypertension, independent of other behavioural and metabolic factors6. Insulin resistance has been identified as a key mechanism linking obesity to hyperuricemia, influencing uric acid metabolism and excretion7. Additionally, weight loss may reduce serum uric acid levels by improving metabolic conditions. However, current research on the associations between different weight change patterns and hyperuricemia is insufficient, particularly with respect to the impact of weight changes from early adulthood to middle age on the later risk of hyperuricemia.
This study explores the associations between different weight change patterns from early adulthood to middle age and the risk of hyperuricemia. By analyzing data from U.S. adults, we intend to assess the impact of weight changes on the risk of hyperuricemia. The findings of this study will provide important epidemiological evidence for the prevention and treatment of hyperuricemia.
Materials and methods
Study population
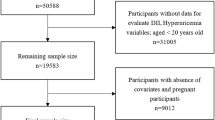
The NHANES employed a complex, multistage, probability sampling method to gather nationally representative health-related data on the U.S. population. Approval for NHANES was obtained from the NCHS Research Ethics Review Board, and all participants provided informed written consent8. In this study, we enrolled participants aged 40–75 years from the baseline survey, including 29,476 from the NHANES (1999–2018) datasets. We excluded pregnant women (n = 31), participants with missing data for BMI at baseline (n = 1613), participants with missing data for BMI 10 years’ prior (n = 910), participants with BMI < 18.5 kg/m2 at baseline or 10 years’ prior (n = 655), and participants with missing data for uric acid (n = 1439), sampling weights of NHANES (n = 1271), and covariates (n = 3012). As a result, 20,545 participants were eligible for further analyses (Fig. 1).

Flowchart of eligible subjects included in this study.
Assessment of weight change
The baseline weight and height were measured in the mobile examination center (MEC). The participants recalled their weights 10 years before baseline. BMI at 10 years before the baseline survey (BMI10prior) and at the baseline survey (BMIbaseline) were computed via the formula weight (kg) divided by the square of height (m2). Based on previous studies9, we categorize weight changes from 10 years before the baseline into six patterns: stable normal pattern (< 25.0 at both times), maximum overweight pattern (25.0–29.9 at either time but not ≥ 30.0 at the other time), obese to normal pattern (≥ 30.0 at younger age and < 25.0 later), obese to overweight pattern (≥ 30.0 at younger age and 25.0–29.9 later), non-obese to obese pattern (< 30.0 at a younger age and ≥ 30.0 later), and stable obesity (≥ 30.0 at both times). The percentage change in BMI from 10 years before the baseline was computed as (BMIbaseline − BMI10prior) / BMI10prior, and expressed as a percentage.
Measurement of serum uric acid and definition of hyperuricemia
The serum uric acid level was determined with a Beckman Synchron LX20 (Beckman Coulter, Inc., Brea, CA, U.S.A) after the conversion of uric acid to allantois and hydrogen peroxide by uricase. Hyperuricemia was defined as serum uric acid ≥ 7.0 mg/dL in males and ≥ 6.0 mg/dL in females10.
Assessment of covariates
Drawing from existing literature9,11, we incorporated demographic variables, lifestyle factors, medical comorbidities, and medication history as covariates gathered at baseline. Demographic variables encompassed age, sex, race/ethnicity (Mexican American, Other Hispanic, non-Hispanic white, non-Hispanic black, and other race), educational attainment (< 9th grade, 9-12th grade, > 12th grade), marital status (married, separated, never married), and family poverty income ratio (PIR) categories (≤ 1.3, 1.3–3.5, and > 3.5). Lifestyle factors comprised the 2015 Healthy Eating Index Score (HEI-2015) (categorized into four equal groups), level of physical activity (sedentary, moderate, or vigorous), smoking status (never, former, or current smoker), and alcohol consumption (yes or no). The medical comorbidities comprised self-reported baseline histories of hypertension, diabetes, cardiovascular disease (CVD), and chronic kidney disease (CKD). Personal histories of hypertension, diabetes, and CVD were ascertained using the following specific question: ‘Have you ever been told by a doctor or other health professional about the conditions listed below?’.Cardiovascular disease (CVD) was identified by the presence of one or more of the following conditions: congestive heart failure, coronary heart disease, angina, heart attack, or stroke. Chronic kidney disease (CKD) was defined as a glomerular filtration rate less than 60 mL/min/1.73m2. The medication history included the use of aspirin, anti-hyperuricemia medications(Allopurinol, Febuxostat, Alloxanthine), and furosemide.
Statistical analyses
Following the NHANES analysis guidelines, the study accounted for complex sampling designs and weights8. Dietary weights were applied for the weighted analysis. A 4-year set of dietary weights (WTDR4YR) was utilized as the data encompassed NHANES 1999–2000 and 2001–2002. For the NHANES 2003–2018 data, the dietary day-1 sample weight (WTDRD1) was employed. The sampling weights for 1999–2018 were determined as WTDR4YR*1/5 for 1999–2002 and WTDRD1*1/10 for the remaining years. Categorical variables are reported as unweighted numbers with weighted percentages, whereas continuous variables are presented as the means and standard deviation. Linear regression analyses were employed for continuous variables, and χ2 tests were utilized for categorical variables to compare variables across groups. No imputation methods were applied, given the small proportion of missing data (ranging from 0% to 7.9% across variables). Multivariable logistic regression models were employed to calculate the odds ratio (OR) and 95% confidence interval (95% CI) to assess the relationship between weight change patterns and hyperuricemia. Model 1 was adjusted for demographic variables (sex, age, race/ethnicity, educational attainment, marital status, and the family poverty income ratio) and the NHANES cycle. Model 2 included the adjustments from Model 1 and lifestyle factors (HEI-2015 score, physical activity, smoking status, and alcohol consumption). Model 3 accounted for the variables in Model 2 and medical comorbidities (hypertension, diabetes, CVD, and CKD). Model 4 encompassed adjustments from Model 3 and medication history (aspirin use, anti-hyperuricemia medications, and furosemide). Furthermore, sensitivity analysis was conducted to enhance result robustness. The logistic regression models treated the weight change patterns as a categorical variable. Interaction and subgroup analyses were carried out to evaluate whether the relationships between weight change patterns and hyperuricemia remained stable across different population groups based on sex, age categories (40–60 vs. 60–75 years), alcohol consumption status (yes vs. no), presence of hypertension (yes vs. no), diabetes (yes vs. no), and CVD (yes vs. no). Heterogeneity and interactions among subgroups were evaluated through logistic regression models and likelihood ratio tests, respectively. Subsequently,a multivariable-adjusted restricted cubic spline model was created with 3 knots to plot the odds ratio (OR) curves, examining the potential nonlinear relationship between weight changes and hyperuricemia. A two-piecewise logistic regression model was utilized to explore the association between weight change patterns and hyperuricemia, adjusting for confounders specified in Model 4.
To ensure robustness, we repeated all analyses after excluding participants using urate-lowering medications (n = 314). This addressed potential confounding by pharmacological interventions affecting uric acid levels.
All analyses were performed using R-4.2.1 (R Foundation for Statistical Computing, Vienna, Austria) and Free Statistics software version 2.0 (Beijing Free Clinical Medical Technology Co., Ltd.). All statistical tests, including chi-square tests, were conducted as two-sided with a significance level of 0.05.
Results
Characteristics of the study participants
In total, 20,545 patients were included in the analysis dataset, with an average age of 54.9 (SD,9.4) years, and 49% were males. The characteristics of the study participants in terms of the five weight change patterns in the 10 years before baseline are shown in Table 1. Compared with individuals in the stable normal group, those in the other groups were more likely to be male, non-Hispanic black or Mexican American, less educated, financially disadvantaged, physically inactive, former smokers and drinkers, and have a higher percentage of prevalent hypertension, diabetes, cardiovascular disease, or chronic kidney disease. They were less likely to maintain good diet quality and more likely to use aspirin, anti-hyperuricemia drugs, and furosemide.
Associations of weight change patterns with hyperuricemia
Table 2 shows the associations of the five models of weight change patterns across adulthood with hyperuricemia. Compared with those of participants who remained at normal weight, the adjusted OR values for participants experiencing maximal overweight, changing from obese to normal, changing from obesity to overweight, changing from the non-obese to obese, and maintaining obesity in the 10 years before baseline were 2.32(95% CI: 1.93–2.80, P < 0.001), 2.62(95% CI: 1.99–3.46, P < 0.001), 4.17(95% CI: 3.40–5.12, P < 0.001), and 4.72(95% CI: 3.95–5.63, P < 0.001), respectively. Interestingly, changing from obesity to normal weight was 0.41(95% CI: 0.21–0.79, P = 0.008).
Subgroup and interaction analyses
In several subgroups, stratified analysis was performed to assess potential effect modifications on the associations of weight change patterns with hyperuricemia. We found significant interactions with sex. No significant interactions were found in the other subgroups after stratification by age, alcohol consumption, hypertension, diabetes or cardiovascular disease (Fig. 2).

Associations of weight change patterns with hyperuricemia stratified by baseline sex, age, alcohol consumption, hypertension, diabetes and cardiovascular disease. Except for the stratification factor itself, the stratifications were adjusted for sex, age, race, education, marital status, PIR, NHANES cycles, HEI-2015, activity, smoking, alcohol, hypertension, diabetes, CVD, CKD, aspirin, anti-hyperuricemia medications and furosemide. HEI-2015 the 2015 healthy eating index score, CVD cardiovascular disease, CKD chronic kidney disease, PIR family poverty income ratio.
Nonlinear association between BMI change and hyperuricemia
Accordingly, the association of the percentage change in BMI during the 10 years before baseline with hyperuricemia was nonlinear (P < 0.001) in the restricted cubic spline model (Fig. 3). According to two-piecewise regression models, the adjusted OR of hyperuricemia was 6.72 (95% CI, 3.76–12.02, P < 0.001) in participants with a percentage change in BMI ≥ 6%. In contrast, there was no association between BMI change and hyperuricemia in participants with a percentage change in BMI < 6% (Table 3).

Association of the percentage change in BMI during the 10 years’ period before baseline with hyperuricemia. The model was adjusted for sex, age, race, education, marital status, PIR, NHANES cycles, HEI-2015, activity, smoking, alcohol, hypertension, diabetes, CVD, CKD, aspirin, anti-hyperuricemia medications and furosemide. Only 0.5–99.5% of the data was shown. HEI-2015 the 2015 healthy eating index score, CVD cardiovascular disease, CKD chronic kidney disease, PIR family poverty income ratio. The red curve represents the multivariable-adjusted nonlinear dose–response relationship between the percentage change in BMI and the risk of hyperuricemia (odds ratio curve); The blue shaded area indicates the 95% confidence interval of this nonlinear association; The red histogram bars depict the frequency distribution of individuals with hyperuricemia across BMI percentage changes; The green histogram bars represent the distribution of individuals without hyperuricemia; A reference point of 6% was set as the inflection point in the two-piecewise regression analysis.“P for non-linearity†refers to the statistical significance of the non-linear association between BMI percentage change and the odds of hyperuricemia. A value less than 0.05 indicates that the relationship deviates significantly from a straight line, justifying a non-linear (spline) model.
The model was adjusted for sex, age, race, education, marital, PIR, NHANES cycles, HEI-2015, activity, smoke, alcohol, hypertension, diabetes, CVD, CKD, aspirin, anti-hyperuricemia medications and furosemide. HEI-2015 the 2015 healthy eating index score, CVD cardiovascular disease, CKD chronic kidney disease, PIR family poverty income ratio.
Sensitivity analysis: Exclusion of urate-lowering medication users
After excluding urate-lowering medication users, results remained consistent: Effect sizes for weight change patterns were consistent with primary analysis (e.g., stable obesity OR = 4.74 [95% CI: 3.97–5.66], P < 0.001).(Table S1).
Discussion
Our objective was to evaluate the relationship between weight change patterns and the prevalence of hyperuricemia in a large, nationally representative sample of U.S. adults. The findings suggest that sustained weight gain or persistent obesity is associated with an increased likelihood of hyperuricemia. Conversely, individuals transitioning from obesity to a normal weight may experience a reduced risk. A nonlinear association between changes in body mass index (BMI) and hyperuricemia was observed, with more substantial BMI increases showing stronger associations, while minor changes appeared unrelated. Notably, the influence of weight change on hyperuricemia risk seemed to be more pronounced among females, indicating potential sex-specific differences in susceptibility.
Some studies have demonstrated that obesity is strongly associated with elevated uric acid levels12,13. A nationwide study in Korea found that general and abdominal obesity significantly increased hyperuricemia risk5. However, our study offers a unique perspective by examining the relationship between weight changes over a decade and hyperuricemia, diverging from most research that focuses on the associations between baseline BMI or weight and hyperuricemia or gout. Although our design does not allow for the determination of causality as a cohort study would, it captures a critical aspect of weight dynamics over time, which is often overlooked in traditional cross-sectional analyses.
We also observed an association between weight reduction to a normal range and a decreased risk of hyperuricemia, a finding not commonly reported in previous studies, possibly highlighting the importance of weight management in preventing hyperuricemia. Studies from different countries or regions, such as one from Korea, also support the relationship between weight change and the risk of hyperuricemia14, aiding in understanding the global prevalence of this relationship.
By analyzing data from a nationally representative sample of U.S. adults, our study provides insights into how variations in weight over 10Â years are linked to hyperuricemia. This relationship has not been fully explored in studies considering only a single time point. This approach emphasizes the importance of long-term weight trends rather than static measures, potentially influencing the development of hyperuricemia.
In this study, the impact of weight change on hyperuricemia was more pronounced in females than in males, a finding that is consistent with several previous studies. Estrogen fluctuations are critical in explaining this effect. Estrogen regulates fat metabolism15,16 and influences renal uric acid excretion17, which could lead to greater fluctuations in uric acid levels during weight changes in females. Additionally, fat distribution differs between males and females, with women typically storing fat in the lower body and men storing it in the abdominal area. This difference in fat distribution could affect the role of adipose tissue in uric acid metabolism18,19. Moreover, women are more susceptible to metabolic changes such as insulin resistance due to obesity, which may exacerbate the onset of hyperuricemia after weight gain20.Although our study identified a stronger weight-hyperuricemia association in females, the cross-sectional design cannot preclude bidirectional effects. For instance, hyperuricemia may reduce physical activity, exacerbating weight gain, while perimenopausal weight fluctuations in women may coincide with estrogen decline to jointly alter uric acid levels. Longitudinal studies with repeated measurements of both weight and uric acid are warranted to disentangle causality.
A significant nonlinear relationship was observed between BMI percentage changes and hyperuricemia risk. The findings suggest that only substantial weight changes, particularly those involving marked increases in BMI, may meaningfully influence uric acid levels. In contrast, relatively minor fluctuations in BMI appear to have little to no impact. This highlights the importance of weight change in determining metabolic risk, reinforcing the need for effective weight management strategies in hyperuricemia prevention. This is consistent with some existing studies21,22. Studies have shown that weight loss of 10Â kg or more is associated with a higher likelihood of achieving norm glycemia, with odds ratios increasing significantly with greater weight loss21. Bariatric surgery leads to rapid weight loss and significant fluctuations in sUA, with initial drops followed by temporary increases, ultimately stabilising at lower levels23,24. Moreover, this nonlinear relationship between weight change and sUA level suggests a threshold effect. Factors such as baseline sUA levels and metabolic responses can influence the degree of uric acid reduction, indicating that individual responses to weight loss may vary22.
The relationship between weight gain and hyperuricemia may involve several physiological mechanisms. First, adipose tissue plays a critical role in uric acid metabolism25. In obese individuals, adipose tissue secretes pro-inflammatory cytokines, which not only promote uric acid synthesis. Nevertheless, it may also inhibit renal uric acid excretion, increasing serum uric acid levels. Second, obesity is often associated with insulin resistance, exacerbating uric acid accumulation because insulin resistance is closely linked to reduced renal uric acid excretion26,27. Furthermore, the low-grade chronic inflammation induced by obesity is one of the key factors driving hyperuricemia, as chronic inflammation stimulates uric acid production and inhibits its excretion28,29.
Our research possesses distinct advantages, such as a substantial number of participants, extensive detail in covariate data, and the implementation of sensitivity assessments. These elements contribute to a more precise and applicable comprehension of the link between patterns of weight fluctuation and elevated uric acid levels. One of the main limitations of this study is its retrospective cross-sectional design, we are unable to assess whether hyperuricemia occurs before or after the weight change and thus cannot determine its causal relationship. Additionally, the data relied on self-reports, which may introduce information bias, especially in reporting weight changes, as participants may underreport or over-report their weight fluctuations. Although multiple adjustments for confounding factors were made in the analysis, residual confounding could not be entirely ruled out. Therefore, future prospective studies are needed to confirm these findings and further explore the long-term effects of weight changes on hyperuricemia.
Our study thoroughly investigated the nonlinear relationship between weight change and hyperuricemia, with a significant impact on uric acid levels only observed with a BMI change of ≥ 6%. Notably, the influence of weight change on hyperuricemia was more pronounced in women than in men, underscoring the importance of gender differences in weight management. These findings provide a new perspective on the prevention of hyperuricemia.
Data availability
Further inquiries can be directed to the corresponding author.
References
Singh, A., Debnath, R. & Chawla, V. P A Chawla Heterocyclic compounds as xanthine oxidase inhibitors for the management of hyperuricemia: Synthetic strategies, structure–activity relationship and molecular docking studies (2018–2024). RSC Med. Chem. 15, 1849–1876 (2024).
Chen-Xu, M., Yokose, C., Rai, S. K., Pillinger, M. H. & Choi, H. K. Contemporary Prevalence of Gout and Hyperuricemia in the United States and Decadal Trends: The National Health and Nutrition Examination Survey, 2007–2016. Arthritis Rheumatol. 71, 991–999 (2019).
Chen, Y., Luo, L., Hu, S., Gan, R. & Zeng, L. The chemistry, processing, and preclinical anti-hyperuricemia potential of tea: A comprehensive review. Crit. Rev. Food Sci. Nutr. 63, 7065–7090 (2023).
Karantas, I. D., Miliotou, A. N. & Siafaka, P. I. An updated review for hyperuricemia and gout management; Special focus on the available drug delivery systems and clinical trials. Curr. Med. Chem. 31, 5856–5883 (2024).
Bae, J., Park, K.-Y., Son, S., Huh, Y. & Nam, G. E. Associations between obesity parameters and hyperuricemia by sex, age, and diabetes mellitus: A nationwide study in korea. Obes. Res. Clin. Pract. 17, 405–410 (2023).
Hong, C. et al. Elevated uric acid mediates the effect of obesity on hypertension development: A causal mediation analysis in a prospective longitudinal study. Clin. Epidemiol. 14, 463–473 (2022).
Cheng, L. et al. The associations of insulin resistance, obesity, and lifestyle with the risk of developing hyperuricaemia in adolescents. BMC Endocr. Disord. 24, 220 (2024).
Liu, H., Wang, D., Wu, F., Dong, Z. & Yu, S. Association between inflammatory potential of diet and self-reported severe headache or migraine: A cross-sectional study of the national health and nutrition examination survey. Nutrition 113, 112098 (2023).
Chen, C., Ye, Y., Zhang, Y., Pan, X.-F. & Pan, A. Weight change across adulthood in relation to all cause and cause specific mortality: Prospective cohort study. BMJ 367, l5584 (2019).
Zhang, Y.-Y., Qiu, H.-B. & Tian, J.-W. Association Between Vitamin D and Hyperuricemia Among Adults in the United States. Front. Nutr. 7, 592777 (2020).
Bai, L., Zhou, J.-B., Zhou, T., Newson, R. B. & Cardoso, M. A. Incident gout and weight change patterns: A retrospective cohort study of U.S. adults. Arthritis Res. Ther. 23, 69 (2021).
Mao, T., He, Q., Yang, J., Jia, L. & Xu, G. Relationship between gout, hyperuricemia, and obesity-does central obesity play a significant role?-a study based on the NHANES database. Diabetol. Metab. Syndr. 16, 24 (2024).
Ali, N. et al. Prevalence of hyperuricemia and the relationship between serum uric acid and obesity: A study on bangladeshi adults. PLoS ONE 13, e0206850 (2018).
Hwang, J., Lee, M. Y., Ahn, J. K. & Cha, H.-S. Relationship between changing body mass index and serum uric acid alteration among clinically apparently healthy korean men. Arthritis Care Res. 74, 1277–1286 (2022).
Mahboobifard, F. et al. Estrogen as a key regulator of energy homeostasis and metabolic health. Biomed. Pharmacother. 156, 113808 (2022).
Steiner, B. M. & Berry, D. C. The regulation of adipose tissue health by estrogens. Front. Endocrinol. 13, 889923 (2022).
Takiue, Y., Hosoyamada, M., Kimura, M. & Saito, H. The effect of female hormones upon urate transport systems in the mouse kidney. Nucleosides, Nucleotides Nucleic Acids 30, 113–119 (2011).
Zhang, X. et al. Gender difference in the relationship between serum uric acid reduction and improvement in body fat distribution after laparoscopic sleeve gastrectomy in chinese obese patients: A 6-month follow-up. Lipids Health Dis. 17, 288 (2018).
Matsuura, F. et al. Effect of visceral fat accumulation on uric acid metabolism in Male obese subjects: Visceral fat obesity is linked more closely to overproduction of uric acid than subcutaneous fat obesity. Metabolism 47, 929–933 (1998).
Nilsson, P. M., Lind, L., Pollare, T., Berne, C. & Lithell, H. Differences in insulin sensitivity and risk markers due to gender and age in hypertensives. J. Hum. Hypertens. 14, 51–56 (2000).
Zhu, Y., Zhang, Y. & Choi, H. K. The serum urate-lowering impact of weight loss among men with a high cardiovascular risk profile: The multiple risk factor intervention trial. Rheumatol. (Oxf. Engl.) 49, 2391–2399 (2010).
Krzystek-Korpacka, M. et al. The effect of a one-year weight reduction program on serum uric acid in overweight/obese children and adolescents. Clin. Chem. Lab. Med. 49, 915–921 (2011).
Xu, C. et al. Factors Influencing Early Serum Uric Acid Fluctuation After Bariatric Surgery in Patients with Hyperuricemia. Obes. Surg. 31, 4356–4362 (2021).
Lu, J. et al. Effects of bariatric surgery on serum uric acid in people with obesity with or without hyperuricaemia and gout: A retrospective analysis. Rheumatol. (Oxf. Engl.) 60, 3628–3634 (2021).
Rospleszcz, S. et al. Association of serum uric acid with visceral, subcutaneous and hepatic fat quantified by magnetic resonance imaging. Sci. Rep. 10, 442 (2020).
Yoo, H.-G. et al. Prevalence of insulin resistance and metabolic syndrome in patients with gouty arthritis. Rheumatol. Int. 31, 485–491 (2011).
Spatola, L., Ferraro, P. M., Gambaro, G., Badalamenti, S. & Dauriz, M. Metabolic syndrome and uric acid nephrolithiasis: Insulin resistance in focus. Metab. Clin. Exp. 83, 225–233 (2018).
Olexa, P. et al. Uric acid–a marker for systemic inflammatory response in patients with congestive heart failure?. Wien. Klin. Wochenschr. 114, 211–215 (2002).
Bodofsky, S., Merriman, T. R., Thomas, T. J. & Schlesinger, N. Advances in our understanding of gout as an auto-inflammatory disease. Semin. Arthritis Rheum. 50, 1089–1100 (2020).
Acknowledgements
We thank Jie Liu of the Department of Vascular and Endovascular Surgery, Chinese PLA General Hospital, for his contribution to the statistical support, study design consultations, and comments regarding the manuscript.
Funding
Project supported by Peking University International Hospital Research Grant. (grant YN2022QN04).
Author information
Authors and Affiliations
Contributions
YZ: Writing – review & editing, Writing the original draft, Methodology, Funding acquisition, Conceptualization. FL: Data curation, Methodology, Formal Analysis, Writing the original draft. QH:Writing – review & editing. ZZ: Data curation.SL: Writing – review & editing, Methodology. HL: Data curation, Writing – review & editing, Methodology.All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
The studies involving humans were approved by the National Center for Health Statistics (NCHS) Ethics Review Committee. The studies were conducted under local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zou, Y., Li, F., Huang, Q. et al. Associations of weight change patterns with hyperuricemia risk in U.S. adults. Sci Rep 15, 21124 (2025). https://doi.org/10.1038/s41598-025-06276-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-06276-3
