

Temporal and sequence-related variability in diffusion-weighted imaging of presumed cerebrovascular accidents in the dog brain
- PMID: 36419725
- PMCID: PMC9676236
- DOI: 10.3389/fvets.2022.1008447
Temporal and sequence-related variability in diffusion-weighted imaging of presumed cerebrovascular accidents in the dog brain
Abstract
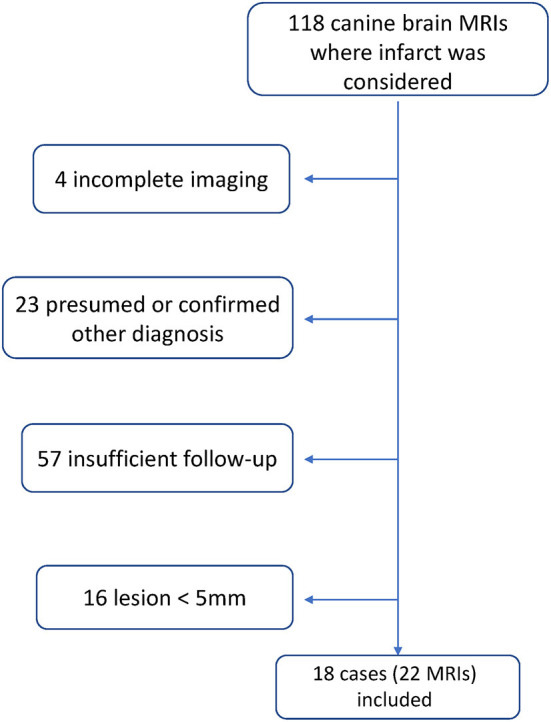
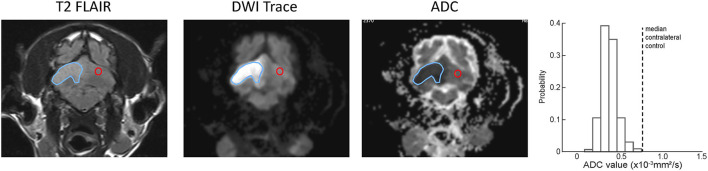
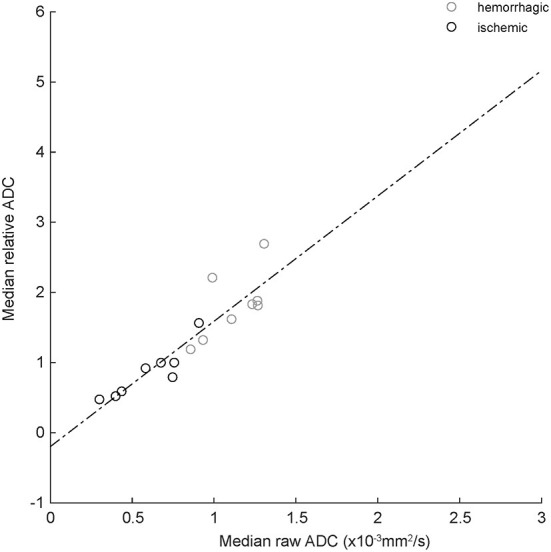
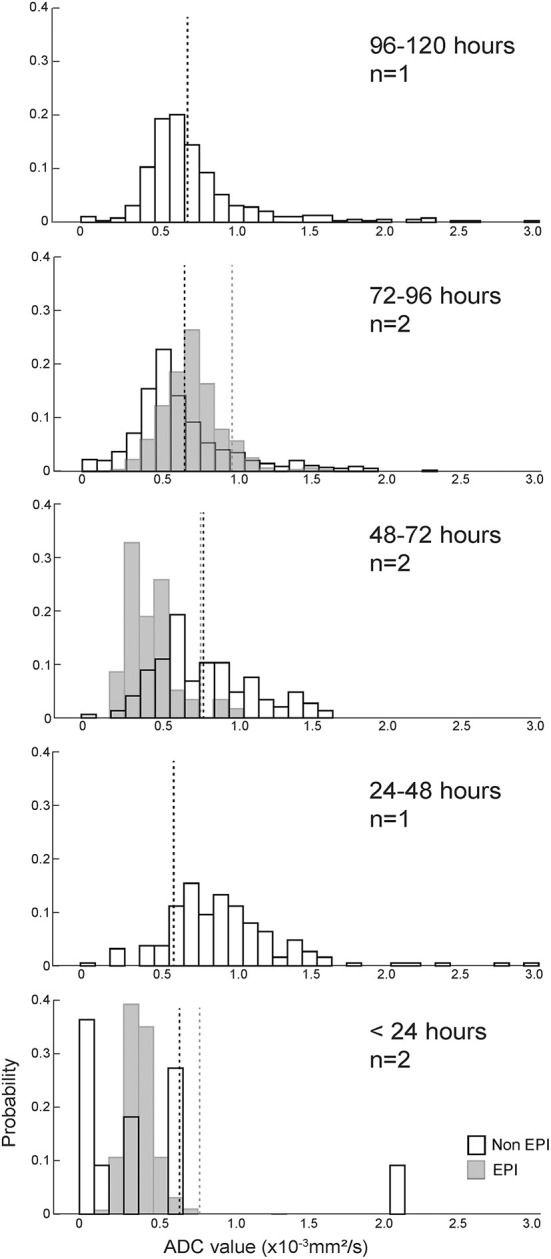
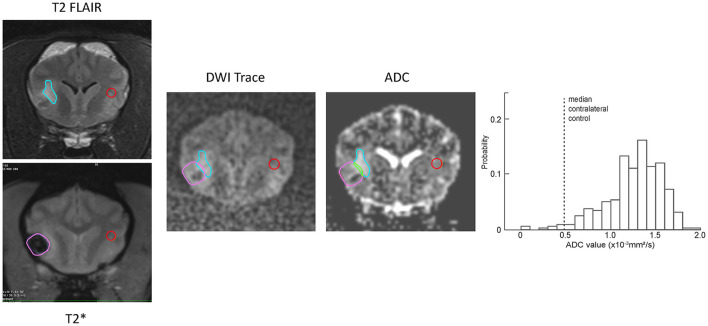
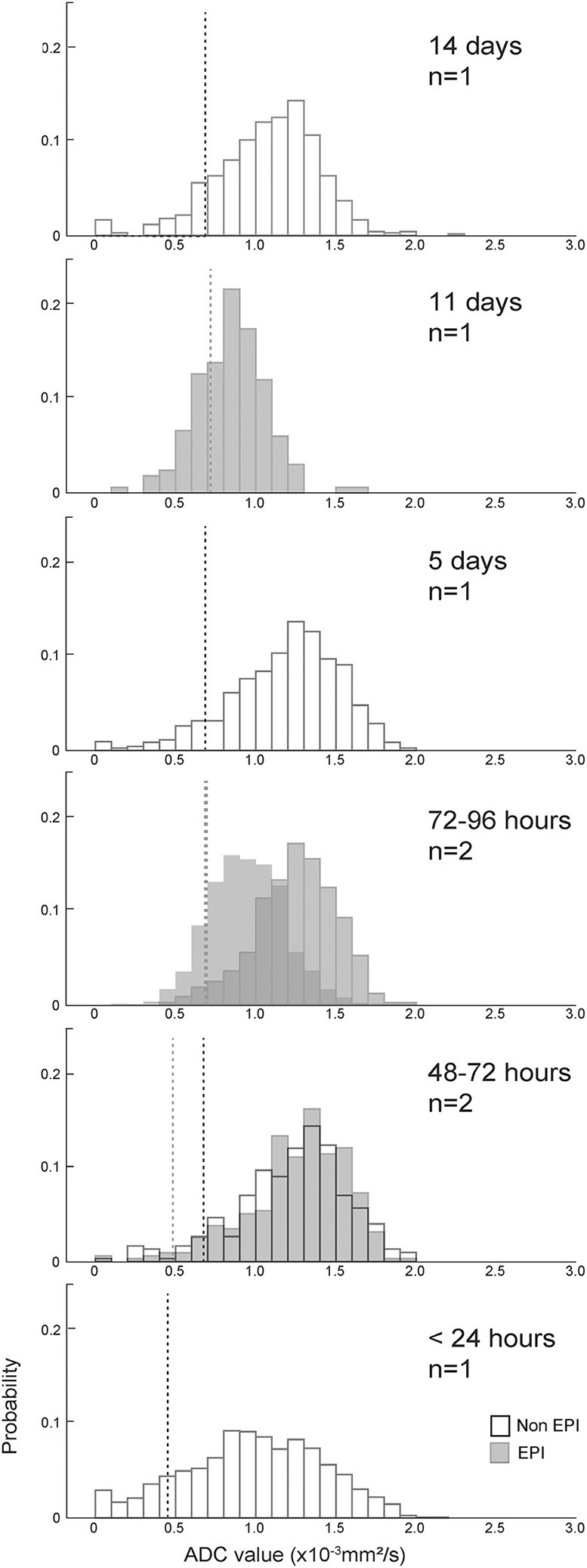
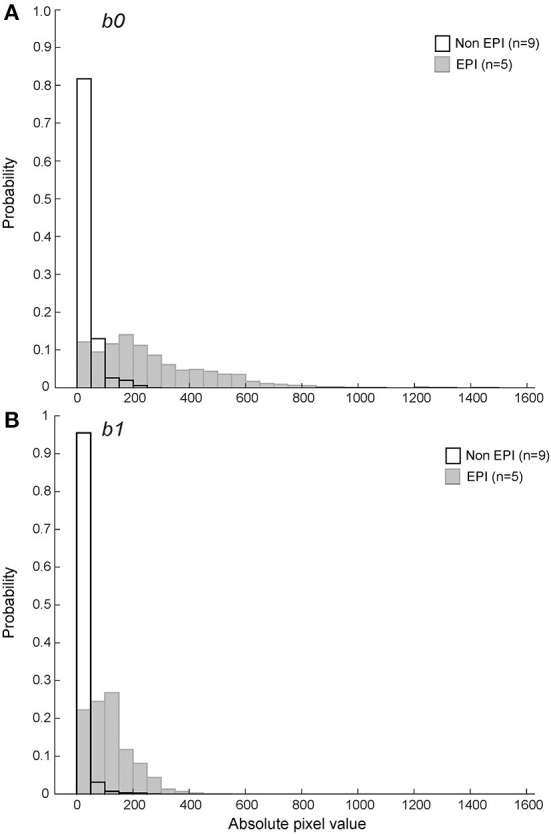
Diffusion-weighted MRI (DWI) is often used to guide clinical interpretation of intraparenchymal brain lesions when there is suspicion for a cerebrovascular accident (CVA). Despite widespread evidence that imaging and patient parameters can influence diffusion-weighted measurements, such as apparent diffusion coefficient (ADC), there is little published data on such measurements for naturally occurring CVA in clinical cases in dogs. We describe a series of 22 presumed and confirmed spontaneous canine CVA with known time of clinical onset imaged on a single 3T magnet between 2011 and 2021. Median ADC values of < 1.0x10-3 mm2/s were seen in normal control tissues as well as within CVAs. Absolute and relative ADC values in CVAs were well-correlated (R2 = 0.82). Absolute ADC values < 1.0x10-3 mm2/s prevailed within ischemic CVAs, though there were exceptions, including some lesions of < 5 days age. Some lesions showed reduced absolute but not relative ADC values when compared to matched normal contralateral tissue. CVAs with large hemorrhagic components did not show restricted diffusion. Variation in the DWI sequence used impacted the ADC values obtained. Failure to identify a region of ADC < 1.0x10-3 mm2/s should not exclude CVA from the differential list when clinical suspicion is high.
Keywords: ADC; MRI; canine; diffusion; ischemia; stroke.
Copyright © 2022 Boudreau, Kerwin, DuPont, Levine and Griffin.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Regional ADC values of the morphologically normal canine brain.Front Vet Sci. 2023 Nov 8;10:1219943. doi: 10.3389/fvets.2023.1219943. eCollection 2023. Front Vet Sci. 2023. PMID: 38026624 Free PMC article.
-
Metabolic counterpart of decreased apparent diffusion coefficient during hyperacute ischemic stroke: a brain proton magnetic resonance spectroscopic imaging study.Stroke. 2003 Jul;34(7):e82-7. doi: 10.1161/01.STR.0000078659.43423.0A. Epub 2003 Jun 19. Stroke. 2003. PMID: 12817104 Clinical Trial.
-
Comparison of the diagnostic performances of diffusion parameters in diffusion weighted imaging and diffusion tensor imaging of breast lesions.Eur J Radiol. 2013 Dec;82(12):e801-6. doi: 10.1016/j.ejrad.2013.09.001. Epub 2013 Sep 13. Eur J Radiol. 2013. PMID: 24099642
-
The role of diffusion tensor imaging in the evaluation of ischemic brain injury - a review.NMR Biomed. 2002 Nov-Dec;15(7-8):561-9. doi: 10.1002/nbm.786. NMR Biomed. 2002. PMID: 12489102 Review.
-
Diffusion-weighted MRI for evaluation of acute stroke.Neurology. 1998 Sep;51(3 Suppl 3):S47-9. doi: 10.1212/wnl.51.3_suppl_3.s47. Neurology. 1998. PMID: 9744834 Review.
Cited by
-
Case Report: Clinical and MRI features of hemorrhagic transformation after ischemic stroke in a dog.Front Vet Sci. 2025 Jun 18;12:1589636. doi: 10.3389/fvets.2025.1589636. eCollection 2025. Front Vet Sci. 2025. PMID: 40607364 Free PMC article.
References
-
- Rivers CS, Wardlaw JM, Armitage PA, Bastin ME, Hand PJ, Dennis MS. Acute ischemic stroke lesion measurement on diffusion-weighted imaging–important considerations in designing acute stroke trials with magnetic resonance imaging. J Stroke Cerebrovasc Dis. (2007) 16:64–70. 10.1016/j.jstrokecerebrovasdis.2006.11.003 - DOI - PubMed
LinkOut - more resources
Full Text Sources